

The Real Reason Nothing Has Worked for Your Reflux
The Real Reason Nothing Has Worked for Your Reflux
A question almost no doctor asks, and why it may explain ten years of failed treatments.

There is one question about your reflux that almost no one has asked you.
Not what triggers it.
Not what you ate.
Not how long you have had it.
The question is this.
What part of your body is actually supposed to stop reflux from happening?
Most people have never been told the answer.
It is a muscle.
A ring of tissue at the top of your stomach, right where your esophagus meets it.
It is called the lower esophageal sphincter, or the LES.
It is not a theory or a signaling pathway.
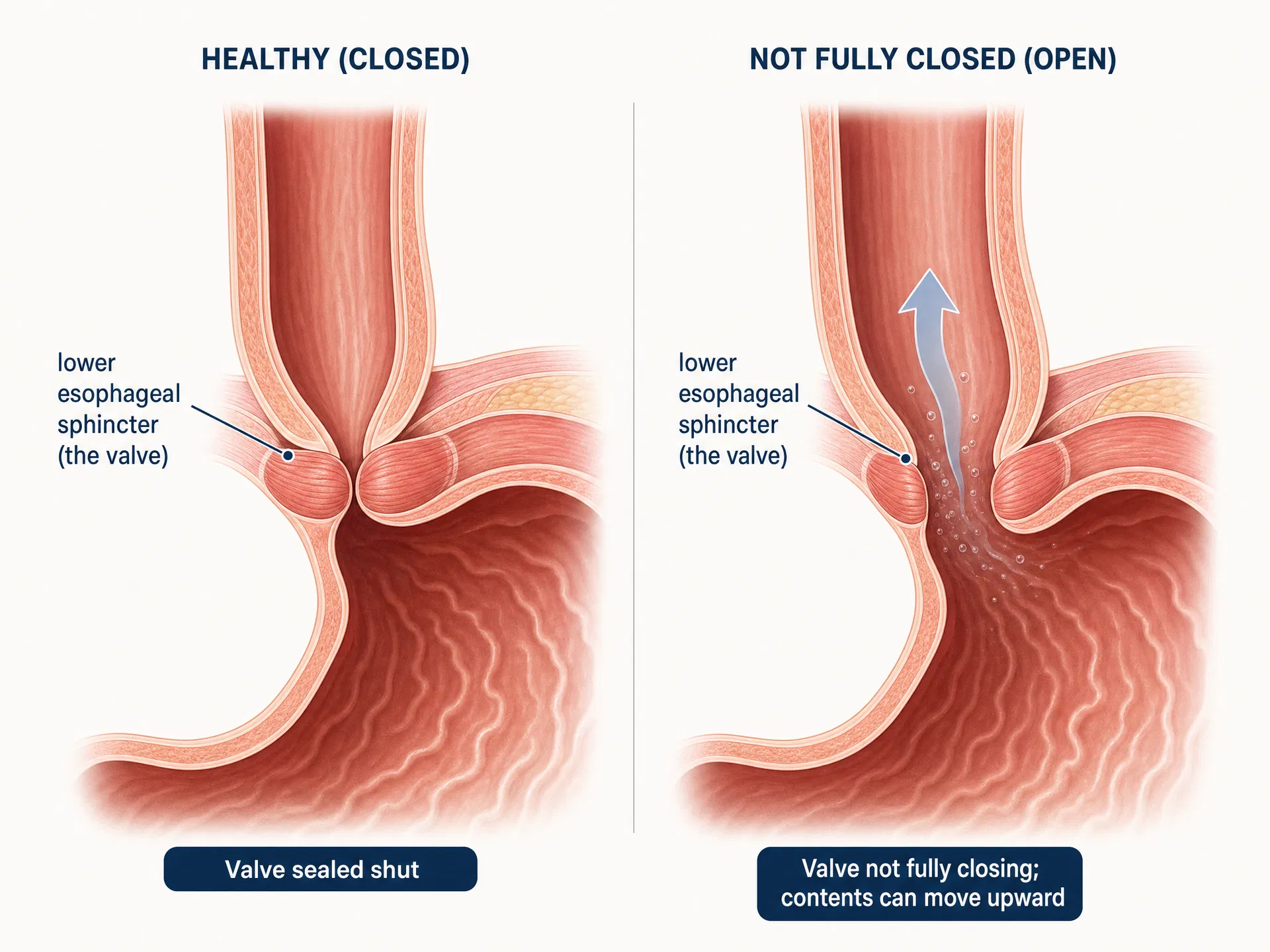
It is a valve.
A door that is supposed to open when you swallow and close when you are done.
And if you have had reflux for more than a year, yours has stopped closing all the way.
That single fact may be the reason nothing you have tried has worked.
This is the part of the story that a gastroenterologist named Dr. Daniel Ross has spent years trying to get people to understand.
His point is simple.
Reflux is a mechanical problem.
A worn valve that no longer seals.
And almost everything the average person has ever been handed for it is a chemical solution.
"For forty years we have been treating reflux as a chemistry problem," Ross says.
"We lower the acid, we neutralize the acid, we block the acid. But the valve that is supposed to hold everything down is still failing. We have been changing the fluid instead of fixing the door."
Once you hear it that way, your own history starts to make sense.
A valve fails for physical reasons.
It weakens with age, the way every muscle does after a certain point.
It gets pushed open from below by pressure, from belly weight, from a large meal, from a tight waistband, from pregnancy.
In many people over fifty, part of the stomach has slipped up through the diaphragm, so the valve can no longer seat correctly.
Decades of small reflux events stretch it a little more each time.
These are all mechanical failures of a mechanical part.
None of them are caused by your stomach making the wrong kind of acid.
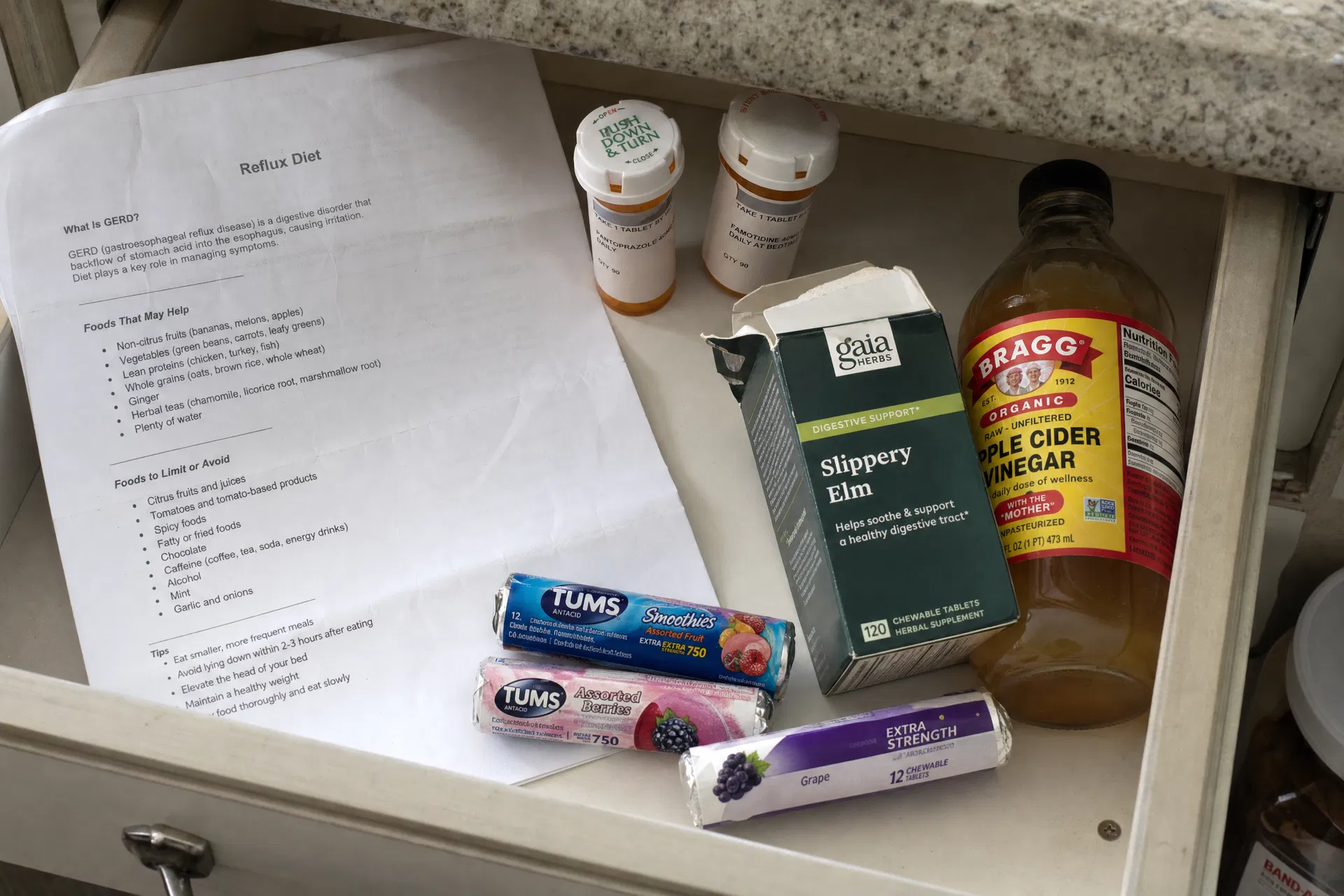
Now look at almost everything you have been offered for it.
Tums and Rolaids neutralize acid for about half an hour.
Pepcid and the other H2 blockers reduce how much acid your stomach makes.
Prilosec, Nexium, and the other proton pump inhibitors shut acid production down at the cellular level.
Apple cider vinegar, digestive bitters, elimination diets, the slippery elm in the cabinet.
Every one of those is doing the same thing.
Every one of them is an attempt to change the fluid.
Not one of them does anything for the door.
You cannot fix a worn valve by changing the chemistry of what flows through it.
Nobody repairs a leaking pipe by adjusting the water.
They fix the pipe.
Here is what the worn valve actually looks like in your life.
You eat dinner and ninety minutes later you feel it rise.
That is the valve letting pressure through.
You lie down and wake at two in the morning with acid in your throat.
That is the valve failing the moment gravity stops helping it.
You take your prescription and the burning eases, but you still feel things come back up after meals.
That is the valve still opening.
There is simply less acid in what passes through, so you notice the splash less.
You lost fifteen pounds one year and felt better.
That was less pressure on the valve.
You have been tracking your triggers for years.
What you have actually been tracking, without knowing it, is the condition of one small muscle.
So why has no one explained this to you before now.
It is not a conspiracy.
It is economics.
Chemical solutions can be patented.
A proton pump inhibitor can be turned into a brand, renewed, and sold for a decade.
A mechanical solution is harder to own.
There is no molecule to protect and no prescription to refill.
So the research money went where the patents were.
Forty years later, the first thing most people are handed for a worn valve is still a drug designed to switch off part of the stomach.
Both the pharmacy and the supplement aisle are making the same mistake.
Both are trying to fix a door with chemistry.
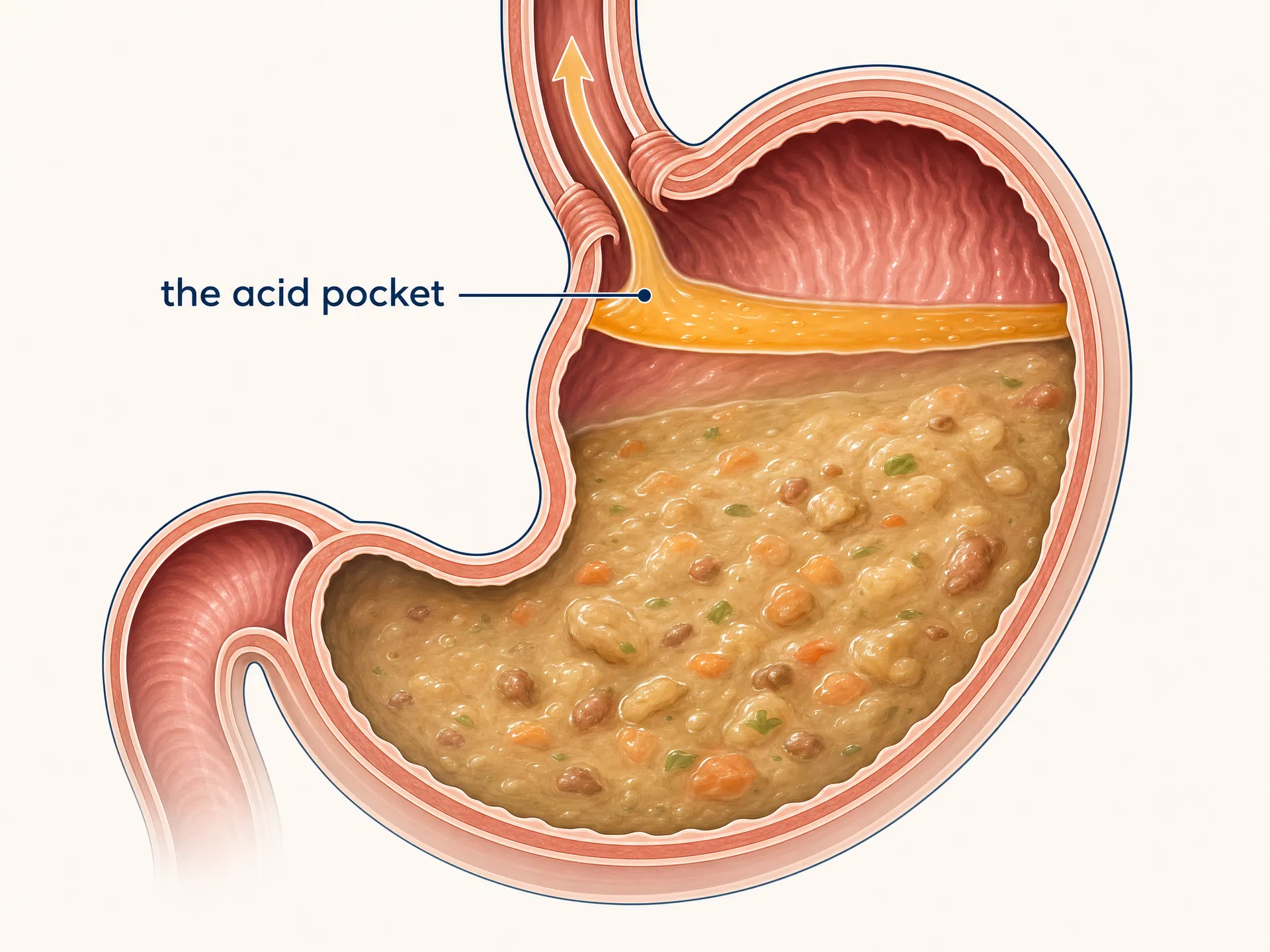
There is one more piece, and it is the part that explains the two in the morning.
After a meal, a layer of acid forms and sits right at the top of the stomach, just below the valve.
Researchers call it the acid pocket.
In a person whose valve seals properly, it stays put.
In a person whose valve does not, that pocket is the first thing to come back up.
This is why the burning is worst right after you eat, and worst again when you lie flat.
You are not imagining the pattern.
You are feeling the acid pocket find the gap in the door.
So here is the logic that follows.
If the problem is mechanical, the answer has to be mechanical too.
Not another way to change the fluid.
A physical barrier that does what the valve has stopped doing.
This is the idea a formula called MendMD was built around.
It is the part of the story Dr. Ross finds most interesting, because it does not try to compete with the drugs on their own terms.
It does something the drugs were never designed to do.
When you take MendMD after a meal, three of its ingredients react with the acid already in your stomach.
Sodium alginate, a fiber from brown seaweed, turns into a soft gel.
Calcium carbonate reacts with the acid and releases tiny bubbles of carbon dioxide.
Sodium bicarbonate speeds that same reaction up.
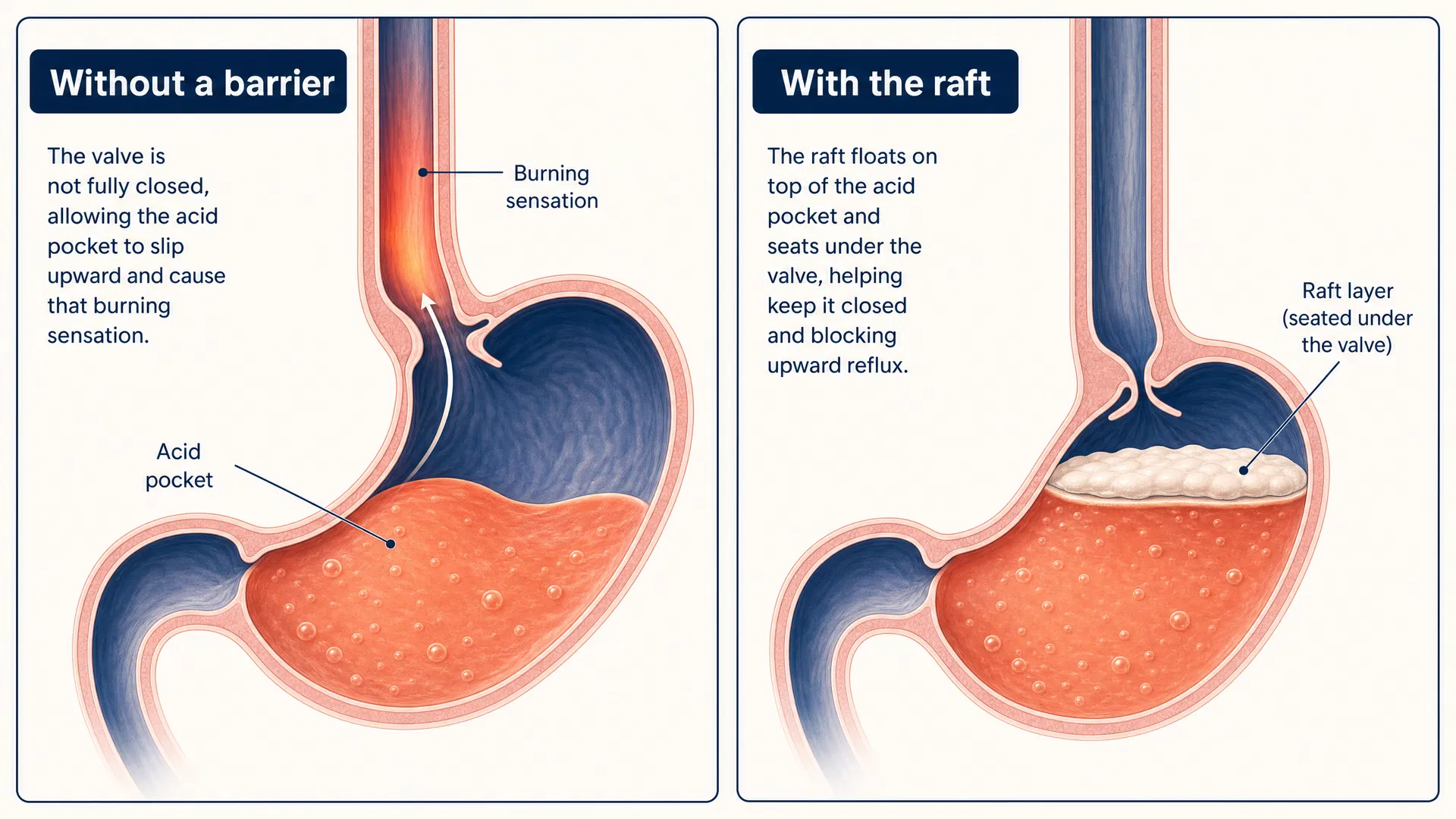
The bubbles get trapped inside the gel and the whole structure becomes buoyant.
It floats to the top of your stomach contents and settles into place right over the acid pocket, exactly where the valve has been failing.
When pressure builds from below, the raft takes it.
When you lie down, the raft stays put.
It is a second layer where your valve used to do the work alone.
This is not a figure of speech.
In imaging studies, researchers have watched the raft form and move to that junction within thirty minutes (Rohof et al., 2013; Sweis et al., 2013).
And because it sits on top of your stomach contents, it never enters your bloodstream.
It does not switch off your acid.
It does not build dependency, and there is no rebound when you stop.
A mechanical problem, met with a mechanical answer.

60-day money-back guarantee
The raft is the part that handles the valve.
But by the time most people read something like this, the reflux has been happening for years, and it has left damage behind.
A thinned protective lining.
Small areas of irritation.
A barrier alone cannot repair that, because healing is a chemical process.
So MendMD pairs the raft with three more ingredients that do that work.
Zinc-L-carnosine, which has been used in Japan for over twenty years to support the stomach lining, binds to irritated tissue and supports its repair.
DGL, a form of licorice, helps your body build back the protective mucus layer that years of acid suppression tend to thin.
Ginger extract helps the stomach empty a little faster, so food moves through instead of sitting and generating the pressure that pushes a weak valve open in the first place.
The brand describes it as three phases.
Shield, repair, and calm.
The raft shields.
The zinc and licorice repair.
The ginger calms the pressure.
It is the first reflux capsule organized around the difference between the mechanical failure and the chemical damage that failure leaves behind.
None of this means a worn valve becomes a young valve overnight.
Dr. Ross is careful about that.
The honest version is that the raft can give relief the same evening you take it, because the barrier is physical and it forms quickly.
The repair side is slower, because tissue heals on its own schedule.
The brand frames the timeline plainly.
In the first few days, the burning after meals may feel calmer as the barrier goes to work.
In the first couple of weeks, the nights tend to settle.
Through weeks three and four, the focus shifts to the lining, and the bloating and pressure often ease.
By the second and third month, the goal is simpler than relief.
It is fewer calculations at dinner, and a quieter stomach you stop thinking about.

60-day money-back guarantee
There is a fair question sitting under all of this.
You have tried things before.
Why would this be different.
The honest answer is the reframe itself.
If everything you tried was aimed at the fluid, then it was never aimed at your actual problem.
That is not a personal failure.
It is a category that has been pointed in the wrong direction for forty years.
The research on the mechanical approach is not thin, either.
In a pooled analysis of randomized trials, alginate raft therapy improved the odds of symptom resolution more than fourfold compared to placebo or antacids (Leiman et al., 2017).
In a head to head trial, it held its own against omeprazole, one of the most prescribed acid drugs in the world (Chiu et al., 2013).
This is not a plant extract hoping to nudge your chemistry.
It is a physical barrier with imaging studies behind it.
As for the other quiet question, the one about why your own doctor never mentioned the valve.
The valve is not a secret.
Any gastroenterologist can describe the lower esophageal sphincter in detail.
The gap is that the standard appointment ends with a prescription for the fluid, because that is the tool the system was built around.
Naming the door, and offering something that sits against it, has simply not been the default.
That is the gap this page exists to close.
If you want to try the mechanical approach for yourself, MendMD is sold directly by the company that makes it.
You can read the full formula and order it here.
https://getmendmd.com/products/mend-md-gut-barrier-repair
A single bottle is 39.99 dollars right now, down from 69.99.
Most people start with the three bottle supply, since the repair side is built to work over two to three months, and shipping is free on more than one bottle.
You take two capsules after your largest meal of the day.
It comes with sixty days to decide.
If it does nothing for you, you email the company and you get your money back.
You have spent years changing the fluid.
This is the first thing on the list that was ever aimed at the door.
60-day money-back guarantee